

 EMERGENCIES 24h. AND APPOINTMENTS
EMERGENCIES 24h. AND APPOINTMENTS 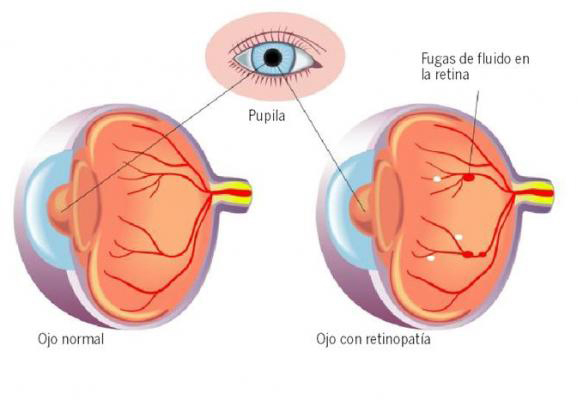
Project Description
Anyone with diabetes is at risk for developing diabetic retinopathy. The longer a person has diabetes, the greater their chance of developing diabetic retinopathy. The condition can develop in anyone who has type 1 or type 2 diabetes.
Early diabetic retinopathy is asymptomatic. Later stages of diabetic retinopathy may cause the following symptoms:
- Blurry or distorted visión
- Fluctuating visión
- Floaters
- Loss of peripheral visión
- Sudden visual loss
Diabetic retinopathy usually affects both eyes.
The longer you have diabetes, the greater your risk of developing diabetic retinopathy. The best way to prevent diabetic retinopathy is through strict control of blood sugar(glucose), blood pressure and blood lipids (cholesterol). It can reduce the risk of developing retinopathy and slow its progression. Since visual loss may not be present in the earlier stages of retinopathy, regular screening of persons with diabetes is essential to enable early intervention.
When to see a doctor
Careful management of your diabetes is the best way to prevent vision loss. If you have diabetes, see your eye doctor for a yearly eye exam with dilation — even if your vision seems fine. Pregnancy may worsen diabetic retinopathy, so if you’re pregnant, your eye doctor may recommend additional eye exams throughout your pregnancy.
Contact your eye doctor right away if your vision changes the longer you have diabetes, the greater your risk of developing diabetic retinopathy suddenly or becomes blurry, spotty or hazy.
Classification of Diabetic Retinopathy
Over time, too much sugar in your blood can lead to the blockage of the tiny blood vessels that nourish the retina, cutting off its blood supply. As a result, the eye attempts to grow new blood vessels. But these new blood vessels don’t develop properly and can leak easily.
The diabetic retinopathy (DR) can be classified into two phases:
-Nonproliferative Diabetic Retinopathy(NPDR)
Nonproliferative DR is the early stage of DR. Recognition of nonproliferative retinopathy allows a prediction of risk of progression, visual loss, and determination of a review interval.
When you have NPDR, the walls of the blood vessels in your retina weaken. Tiny bulges (microaneurysms) protrude from the vessel walls of the smaller vessels, sometimes leaking fluid and blood into the retina. Larger retinal vessels can begin to dilate and become irregular in diameter, as well. NPDR can progress from mild to severe, as more blood vessels become blocked.
Nerve fibers in the retina may begin to swell. Sometimes the central part of the retina (macula) begins to swell (macular edema), a condition that requires treatment.
-Proliferative Diabetic Retinopathy(PDR)
Proliferative diabetic retinopathy (PDR) is an advance and severe stage of DR. In this type, damaged blood vessels close off, causing the growth of new, abnormal blood vessels in the retina, and can leak into the clear, jelly-like substance that fills the center of your eye (vitreous). This stage represents an angiogenic response of the retina to extensive ischemia and capillary closure. Neovascularization has be divided into 2 groups: new vessels on the disc (NVD) and new vessels elsewhere (NVE). Typically NVE grow at the interface of perfused and nonperfused retina.
Eventually, scar tissue stimulated by the growth of new blood vessels may cause the retina to detach from the back of your eye. If the new blood vessels interfere with the normal flow of fluid out of the eye, pressure may build up in the eyeball. This can damage the nerve that carries images from your eye to your brain (optic nerve), resulting in glaucoma.
Macular edema(DME) is an important complication that is assessed separately from the stages of retinopathy, as it can be associated with any of the DR stages and can run an independent course.
-Diabetic Macular Edema
It is important to assess the presence and severity of diabetic macular edema (DME) separately from stages of DR.
Complications
- Vitreous hemorrhage. The new blood vessels may bleed into the clear, jelly-like substance(vitreous) that fills your eye. If the amount of bleeding is small, you might see only a few dark spots (floaters). In more-severe cases, blood can fill the vitreous cavity and completely block your vision.
- Retinal detachment. The abnormal blood vessels associated with diabetic retinopathy stimulate the growth of scar tissue, which can pull the retina away from the back of the eye.
- New blood vessels may grow in the front part of your eye and interfere with the normal flow of fluid out of the eye, causing pressure in the eye to build up (glaucoma).
Initial Patient Assessment
Detailed patient assessment should include a complete ophthalmic examination, including visual acuity and the identification and grading of severity of DR and presence of DME for each eye.
-Patient History
- Duration of diabetes
- Past glycemic control (hemoglobin A1c)
- Medications (especially insulin oral hypoglycemics, antihypertensives, and lipid-lowering drugs)
- Systemic history (e.g., renal disease, systemic hypertension, serum lipid levels, pregnancy)
- Ocular history
-Eye exam
- Visual acuity
- Measurement of intraocular pressure (IOP)
- Gonioscopy when indicated (e.g., when neovascularization of the iris is seen or in eyes with increased IOP)
- Slit-lamp biomicroscopy
- Fundus examination
-Follow-up Examination of Patients with Diabetic Retinopathy
In general, the follow-up history and examination should be similar to the initial examination. The assessment of visual symptoms, visual acuity, measurement of IOP, and fundus examination are essential.
Fluorescein angiography is not needed to diagnose DR, proliferative DR or DME, all of which are diagnosed by means of the clinical exam.
Fluorescein angiography can be used as a guide for treating DME and as a means of evaluating the cause(s) of unexplained decreased visual acuity. Fluorescein angiography can also identify macular capillary nonperfusion or sources of capillary leakage resulting in DME as possible explanations for visual loss.
OCT is the most sensitive method to identify sites and severity of DME.
Patient education& Prevention
- Your ophthalmology should discuss the results of your exam and implications with you.
- Patients with DM but without diabetic retinopathy(DR) should have annual screening eye exams.
- The effective treatment for DR depends on timely intervention, despite good vision and no ocular symptoms.
- Educate patients about the importance of maintaining near-normal glucose levels, near-normal blood pressure and to control serum lipid levels.
- Communicate with the general physician (e.g., family physician, internist, or endocrinologist) regarding eye findings.
- Patients with reduced visual function should be refered for vision rehabilitation and social services.
Treatment of Diabetic Retinopathy
If you have proliferative diabetic retinopathy or macular edema, you’ll need prompt surgical treatment. Depending on the specific problems with your retina, options may include:
- Focal laser treatment, photocoagulation.
This laser treatment can stop or slow the leakage of blood and fluid in the eye.
Panretinal photocoagulation, can shrink the abnormal blood vessels. During the procedure, the areas of the retina away from the macula are treated with scattered laser burns. The burns cause the abnormal new blood vessels to shrink and scar. Your vision will be blurry for about a day after the procedure. Some loss of peripheral vision or night vision after the procedure is possible.
- This procedure uses a tiny incision in your eye to remove blood from the middle of the eye (vitreous) as well as scar tissue that’s tugging on the retina and endophotocoagulation. Surgery often slows or stops the progression of diabetic retinopathy, but it’s not a cure.
- Because diabetes is a lifelong condition, future retinal damage and vision loss are still possible. Even after treatment for diabetic retinopathy, you’ll need regular eye exams. At some point, additional treatment may be recommended.
Researchers are studying new treatments for diabetic retinopathy, including medications that may help prevent abnormal blood vessels from forming in the eye( anti VEGF). Some of these medications are injected directly into the eye to treat swelling or abnormal blood vessels
Patient should be informed:
- Patients usually need numerous follow-up visits and may require supplementary laser treatment.
- PRP reduces the risk of visual loss and blindness.
- Although laser treatment is effective, some patients may still develop vitreous hemorrhage. The hemorrhage is caused by the diabetes and not by the laser; it may mean the patient needs more laser treatment.
- Laser treatment often reduces peripheral and night vision; treatment may moderately reduce central vision.
Treatment for Diabetic Macular Edema
- Optimize medical treatment: Improve glycemic control if HbA1c > 7.5% as well as associated systemic hypertension or dyslipidemia.
- Consider focal laser to leaking microaneurysms. Intravitreal anti- VEGF treatment (e.g., with ranibizumab [Lucentis], bevacizumab [Avastin], or Aflibercept [Eylea]) therapy). Consideration should be given to monthly intraocular injections followed by treatment interruption and re-initiation based on visual stability and OCT. Patients should be monitored almost monthly with OCT to consider the need for treatment.
- DME associated with proliferative DR: combined intravitreal anti-VEGF therapy and panretinal photocoagulation should be considered.
- Vitreomacular traction or epiretinal membrane on OCT: a vitrectomy may be indicated.
- Bevacizumab (Avastin) is an appropriate alternative to raniziumab (Lucentis) or aflicercept (Eyelea). Laser can be applied earlier to areas of persistent retinal thickening in eyes unresponsive to anti- VEGF treatment.
Indications for Vitrectomy
- Severe vitreous hemorrhage of 1–3 months duration and that does not clear spontaneously.
- Advanced active proliferative DR that persists despite extensive panretinal laser photocoagulation.
- Traction macular detachment of recent onset.
- Combined traction-rhegmatogenous retinal detachment.
- Tractional macular edema or epiretinal membrane involving the eye.